


Background
HIVQUAL-Haiti was launched in 2007 with completion of baseline data collection in 2008, along with Organizational Assessments at all 19 initial clinics. Implementation has since expanded to 74 clinics throughout the country.
The data collection process for HIVQUAL-Haiti has been enhanced and facilitated by an electronic medical records (EMR) system used by clinics supported by the Ministry of Health and Population throughout Haiti. The system has been customized to incorporate the HIVQUAL-Haiti indicators, and allow for the automatic generation of HIVQUAL reports. The EMR was developed by ITECH, a PEPFAR partner, in collaboration with CDC-Haiti.
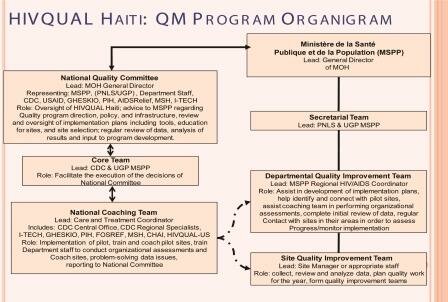
The National Quality Committee - which developed and defined indicators, chose participating facilities and developed an organizational system to support these activities – maintains oversight of the national program. The Committee and HQ-Haiti have confirmed an operational plan for coaching and mentoring which includes 2 coaching visits per year, an annual organizational assessment, and regular communication with facilities to support and collect QI project information.
Despite severe disruptions in service (and in some cases complete termination of services at certain facilities) due to the 2010 earthquake, the HIVQUAL-Haiti team has continued to implement the HQ model to improve quality of care for adults and children living with HIV/AIDS. The in-country team is also currently planning regional trainings to support on-going improvement activities.
HIV/AIDS Epidemic
Haiti has the most significant HIV/AIDS burden in the Caribbean. The prevalence rate in adults aged 15-49 was 2.2% in 2006. Haiti’s epidemic has partly been fueled by high poverty, illiteracy, internal migration, and sexually transmitted infections. Out of a total population of 10,085,214 people, 111,000 people 15 years and older and 12,000 people under 15 years are HIV infected. The life expectancy at birth is 61(58.1) years and the infant mortality rate is 6%(8.6%). Prevalence rates amongst females age 15-24 is 1.4% (2.1% - 2009) while prevalence rates amongst males in the same age group is 0.6%
Demographic Data
Population: ~10 million cf. Rapport de situation nationale a l’intention de l’UNGASS. MARS 2010
- HIV prevalence:
- -250,000 adult and pediatric population (with 123,858 enrolled in care)
- TB/HIV prevalence: ~ 23% of TB patients have HIV
- Other pertinent Demographics: About half (61,0000 of HIV+ are eligible for ART
- About half of the eligible for ART (32,000) are on ART
- Year Program Began: September 2007
- Scope: HIV, pediatrics and PMTCT
- Prevalence in Pregnancy women : 2.5%
- Orphan due to AIDS : 93,000
- Number of HIVQUAL facilities: 57 (as of December 2011)
Haiti Health System Infrastructure
The Haitian health system is composed of public, semi-public and private sector entities. The Ministry of Health is organized into central, departmental and community levels. One third of the nation’s 663 health institutions fall under the auspices of the public sector. Political transitions have represented a significant challenge to the public health care system.
The semi-public sector is made up primarily of non-governmental organizations staffed by the public sector but managed by private entities.
The majority of private health facilities and private physicians, nurses and other health care personnel are centered in the capital, Port-au-Prince.
Coordination of Haiti’s HIV/AIDS response is under the direction of the Ministry of Health. Towards the end of 2008, Haiti initiated a strategic approach to engage key ministries other than the Ministry of Health—such as the ministries of Justice, Youth and Sports, Women, Social Affairs and Education. These ministries were made aware of the existing plan to address HIV/AIDS in the country and were encouraged to develop plans that would align their areas of action to the national HIV/AIDS efforts. Civil society has also played a key role in confronting the HIV/AIDS epidemic in Haiti by providing essential services during times of weakened government capacity.
In 2006, Haiti set goals to increase access to HIV prevention, treatment, care, and support. After setting these goals the country started taking steps towards universal access to care. One of these steps was increasing the number of sites throughout the country that provide ART. The number of sites providing ART increased from 20 sites in 2005 to 75 sites in 2012. As a result, total ART coverage increased from 22% in 2005 to 33% in 2006 to 41% in 2011. The number of HIV infected women receiving ART to prevent mother to child transmission of HIV also increased from 17% in 2005 to 22% in 2007 to 83% in 2011. The rates of ART coverage continued to increase throughout 2012.
References: Accessed 7/16/10
http://www.unaids.org/en/CountryResponses/Countries/haiti.asp
http://apps.who.int/globalatlas/predefinedReports/EFS2008/full/EFS2008_HT.pdf
http://data.unaids.org/pub/FactSheet/2008/sa08_hai_en.pdf
http://www.mesi.ht





Overview
- HQ-Haiti has submitted 13 rounds of data reviewing care provided from January 1, 2008 through March 31, 2014
- 106 HQ-Haiti clinics have participated in HIVQUAL data collection, representing 74% of 143 HIV clinics and 12% of 908 health facilities in-country
- Performance rates have been measured for the following 10 indicators: clinical visits, CD4 monitoring, ARV Therapy, adherence assessment, CPT, TB clinical screen, nutrition evaluation, immunization, PMTCT ARV prophylaxis and family planning
- HIVQUAL Haiti indicators are programmed directly into a fully integrated national electronic medical record system
